|
Addressing Behavioral Health Needs of Men: Substance Abuse > Chapter 1 - Introduction
|
|
 Addressing the Behavioral Health Needs of Men: Substance AbusePresented by
ApprovalsUpon completion of this course the participant will receive 20 CE Credits/Contact Hours. CALIFORNIA: This course meets the criteria and is accepted by the California Board of Behavioral Sciences for continuing education hours for Social Workers, Marriage and Family Therapists, Professional Counselors, and Educational Psychologists. (See Nursing Approval below) TEXAS: This course meets the criteria for acceptable continuing education as defined by the Texas State Board of Professional Counselors, Marriage and Family Therapists and Social Workers. Note: The CA BBS and TX Boards no longer directly approve providers of continuing education; however, this course meets their criteria for acceptable continuing education. This course is accepted/approved by the following for continuing education credits/contact hours:
The California Board of Registered Nursing # CEP 14462
The National Board for Certified Counselors (NBCC) # 6412
The Florida Board of Clinical Social Work, Marriage and Family Therapy and Mental Health Counseling #50-14000 The California Consortium of Addiction Programs and Professionals: CCAPP-IE Provider # 1N-16-256-0824 The California Associations of Alcohol and Drug Educators (CAADE) #CP40 977 H 0425
Objectives1)Recognize the ways in which male gender roles influence men’s psychosocial adaptation, substance use/abuse, and help-seeking behaviors.
2)Identify areas of screening and assessment of substance use disorders. 3)Define three parts of a comprehensive screening and assessment process. 4)Explain the treatment issues for Men. 5)Define co-occurring Physical health problems,behavioral and mental disorder in men from different age groups,diverse culture and geographic groups. 6)Define men’s treatment needs in the context of different modalities and settings and strategies. What is a TIP?This course is part of the “Treatment Improvement Protocols (TIPs) [that] are developed by the Substance Abuse and Mental Health Services Administration (SAMHSA) within the U.S. Department of Health and Human Services (HHS). TIPs are best practice guidelines for the treatment of substance use disorders. TIPs draw on the experience and knowledge of clinical, research, and administrative experts to evaluate the quality and appropriateness of various forms of treatment. TIPs are distributed to facilities and individuals across the country. Published TIPs can be accessed via the Internet at http://kap.samhsa.gov.
Although each TIP strives to include an evidence base for the practices it recommends, SAMHSA recognizes that the field of substance abuse treatment is continually evolving, and research frequently lags behind the innovations pioneered in the field. A major goal of each TIP is to convey front-line information quickly but responsibly. If research supports a particular approach, citations are provided. “ Recommended CitationSubstance Abuse and Mental Health Services Administration. Addressing the Specific Behavioral Health Needs of Men. Treatment Improvement Protocol (TIP) Series 56. HHS Publication No. (SMA) 13-4736. Rockville, MD: Substance Abuse and Mental Health Services Administration, 2013.
1. Creating the ContextIntroductionThis Treatment Improvement Protocol (TIP) examines the history and theories of male socialization, changes in perceptions of masculinity and male roles, fatherhood, and other factors related to men’s substance use, abuse, and treatment. It emphasizes the fact that there is no single concept of masculinity or male identity appropriate for all men. Many factors besides gender status influence men’s identities—age and cultural background, for example, affect how men view what it means to be male. While recognizing that there is tremendous variation among men, this TIP also discusses how American cultural norms shape the way many men evaluate themselves and how this relates to patterns of substance use or abuse and to treatment provided by behavioral health counselors.
Historically, substance abuse treatment services were developed with male clients in mind because most admissions to substance abuse treatment programs were—and are—men. More recently,though there are still more specialized programs and interventions for women than for men (Substance Abuse and Mental Health Services Administration [SAMHSA], Office of Applied Studies [OAS] 2007d), the gender studies and men’s studies fields have begun to identify possible improvements in treatment services for men. Men and women abuse substances for many reasons—some gender-related, some not. Reasons overlap in many areas but markedly diverge in others, necessitating different treatment options. This TIP and TIP 51, Substance Abuse Treatment: Addressing the Specific Needs of Women (Center for Substance Abuse Treatment 2009c), explore gender-specific treatment needs and services that can address those needs. Note: TIPs referred to in this and subsequent chapters are available at the Knowledge Application Program Website (http://kap.samhsa.gov). This chapter explains key issues, such as gender, sex, gender role conflict/stress, and conceptual frameworks relevant to behavioral health services for men with substance use disorders. It also describes concepts of masculinity and associated beliefs. It concludes with discussions of specific patterns of male substance use and abuse and how certain substances affect men differently than women; the current state of male-specific substance abuse treatment; and how this TIP is useful for various audiences of behavioral health service providers. Although this TIP focuses on men with substance use disorders who are receiving treatment in substance abuse treatment settings,much content is directly applicable to clients with other behavioral health problems and disorders or who have a substance use disorder and a co-occurring mental disorder. The content of the TIP is directly applicable in various settings beyond substance abuse treatment programs, including mental illness treatment programs; criminal justice, vocational, and social rehabilitation programs; settings that primarily address physical health or family issues;and housing programs. Defining Sex and GenderOne’s sex is generally assigned according to biological markers. Individuals are typically classified as male or female based on their reproductive organs, but assigning sex based on observable physical or biochemical traits leaves some individuals unassigned due to genital,chromosomal, or hormonal ambiguities.
Gender , on the other hand, is a sociocultural construct that defines expected characteristics of men and women. Femininity refers to characteristics ascribed to women, whereas masculinity refers to characteristics ascribed to men. Gender is not absolute; masculine behavior in one culture can be the opposite in another. Moreover, notions of gender-appropriate behavior change over time and according to context. For example, in the 19th and early 20th centuries, it was considered appropriate for young boys to wear dresses. Notions of gender-appropriate occupations have also changed. For example, when the typewriter was first invented, male clerks were thought to have innate typing abilities far surpassing those of women. However, those stereotypes changed and in a few decades, working as a typist was considered a female occupation.Nursing, long considered a feminine job, has attracted more men in recent years. [Question #1. A sociocultural construct that defines expected characteristics of men and women] In this TIP, masculinity is defined broadly to include commonly accepted expectations for men in the United States. A number of variables can alter accepted ideas about masculinity: economic status, occupation, geographic location, religious affiliation, education, race,ethnicity, and sexuality, among others. Some men are at odds with dominant notions of masculinity; others embrace such notions. Regardless of individual definitions of masculinity, ideas about gender roles and expectations can affect substance abuse treatment for men. A person’s gender identity must also be considered in discussions of masculinity. Gender identity is usually defined as a subjective, continuous, and persistent sense of oneself as male or female, but the importance of gender identity varies from one individual to another. Defining Substance Abuse and DependenceUnless otherwise noted, in this TIP, substance abuse and substance dependence refer to all varieties of substance use disorders described in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision (DSMIV-TR; American Psychiatric Association[APA] 2000). The DSM-IV-TR states that “the term substance can refer to a drug of abuse, a medication, or a toxin”—alcohol is included as a substance as well (p. 191). The text also notes that “many prescribed over-thecounter medications can also cause a sub-stance-related disorder” and that “a wide range of other chemical substances can also lead to the development of substance-related disorders” (p. 191).
Substance dependence is “a cluster of cognitive,behavioral, and physiological symptoms indicating that the individual continues use of the substance despite significant substance-related problems…[in which] there is a pattern of repeated self-administration that can result intolerance, withdrawal, and compulsive drug-taking behavior” (APA 2000, p. 192). Though not a criterion, “craving (a strong subjective drive to use the substance) is likely to be experienced by most (if not all) individuals with substance dependence” (p. 192). [Question #2. A pattern of repeated drug self-administration that can result in tolerance for the drug , withdrawal, and compulsive drug-taking behavior is] According to the DSM-IV-TR (APA 2000),the essential feature of substance abuse is a “maladaptive pattern of substance use manifested by recurrent and significant adverse consequences related to the repeated use of substances” (p. 198). The text notes that, “unlike the criteria for substance dependence, the criteria for substance abuse do not include tolerance, withdrawal, or a pattern of compulsive use and instead include only the harmful consequences of repeated use” (p. 198). It specifies that “the term abuse should be applied only toa pattern of substance use that meets the criteria for this disorder; the term should not be used as a synonym for ‘use,’ ‘misuse,’ or ‘hazardous use’” (p. 198). Although there is general agreement that intensive substance abuse treatment is best provided in specialized substance abuse treatment programs, many men with substance use disorders enter and may continue care in a variety of other behavioral health settings. As a result, in both specialized substance abuse treatment programs and other settings, clients may be seen by behavioral health service providers from a number of disciplines, including substance abuse counselors, mental health counselors, psychologists, social workers, professional counselors, ministers and chaplains, physicians,and persons working in criminal justice settings. The general principles discussed in this TIP will be informative for the broader range of behavioral health specialists who work with men who have substance use disorders. [Question #3. Maladaptive pattern of substance use manifested by recurrent and significant adverse consequents related to the repeated use of substance] Conceptual Frameworks of Masculinity and Male RolesAlthough no one set of behaviors or traits defines masculinity, certain characteristics or expectations are associated with masculinity in abroad range of cultural contexts and across different age groups. Brannon (2005) reviews research on the cross-cultural applicability of gender stereotypes and notes that although diverse cultures label certain characteristics differently as masculine or feminine, there are generally more similarities than differences in gender stereotypes across cultures.
The stereotypical roles that define men with in a culture are referred to as masculinity ideologies (Good et al. 1994). Ideologies are systems of values, beliefs, or ideas shared by a social group and often presumed to be natural or innately true. Masculinity ideologies, then, are a body of socially constructed ideas and beliefs about what it means to be a man and against which men are measured by their societies (Addis and Mahalik 2003; Good and Sherrod 2001). Masculinity ideologies also affect how men think and feel about themselves, and they influence male roles in a society (Pleck 1981,1995). Men internalize these concepts from a nearly age. Through a process of “masculine role socialization,” boys learn how they are expected to act, feel, and think, and they often face negative consequences if they fail to meet those expectations (Addis and Mahalik 2003;Eisler 1995; Good and Sherrod 2001). Scholars have built upon Brannon’s blueprint for masculinity (1976) to classify common,socially accepted male roles (e.g., Levant et al.1992; Mahalik et al. 2003b; Mahalik et al. 2005; Pollack 1998b; Smiler 2004). Individual men may identify with several roles or none and may place more emphasis on some roles than others. The next sections examine specific masculinity concepts and their potential relation to substance abuse; these concepts exist on a continuum and may change over time. [Question #5. A systems of values, beliefs, or ideas shared by a social group and often presumed to be natural or innately true?] Rituals, Rites of Passage, and Alcohol AbuseRituals are socially supported events individuals and families use to mark transitions in their lives. The use of rituals is common to all cultures, although specific rituals vary. As Imber-Black (2002) notes, “human beings are ritual makers. Differing from mere routines in daily life, rituals enable individuals, families, and cultures to create and derive meaning through their symbols and symbolic actions” (p. 445).
The potentially beneficial aspects of rituals are considerable. Rituals can reduce anxiety and foster change (Schwartzman 1982), facilitate development of individual identity and attachment to important values and beliefs of one’s culture, and contribute to “a shared and necessary sense of belonging” (Wolin and Bennett 1984, p. 402). However, rituals can also be harmful—and certain rituals may harm men differently than women. For centuries, men have been indoctrinated into manhood through highly ritualized rites of passage. Most cultures (Gilmore 1990) expect men to prove their worth through dangerous, painful tests of bravery. In the United States, men are often called on to prove their masculinity through sports competitions, high speed driving, or sexual conquests. Many such conventional manhood rituals are intertwined with excessive alcohol consumption, with alcohol acting as a lubricant for the behaviors or an end in itself. Indeed, some researchers who examined binge drinking among college students found drinking to be a form of ritualized behavior (Treise et al. 1999). Critical transitions in men’s lives—adulthood,marriage, fatherhood, retirement, deaths—often go hand in hand with excessive alcohol use, especially in the absence of clear guidance or preparation for the change. Although life transitions are ideal times for men to give comfort and support to each other (those who have made the journey already are especially equipped to do so), this rarely happens (Brooks 1995). Far too frequently, alcohol is substituted for open communication and caring. For example, on reaching legal adulthood at age 21, many men celebrate by getting drunk. Job promotions and sports victories are likewise frequently accompanied by drinking,often to excess. The traditional celebration of the transition from bachelorhood to marriage also often involves alcohol and drug use,which many times drowns out a real need for connection and communication among men. To reduce alcohol consumption among men,the development of new celebrations and rituals that do not include alcohol consumption is necessary. Such changes will take time and effort, but people in recovery already make use of rituals to help them get and remain abstinent. For example, 12-Step groups typically involve quite a few rituals (e.g., opening and closing meetings, celebrating anniversaries,welcoming new members, passing the hat for contributions, giving out small objects such as key chains or coins to symbolize milestones),and these rituals are important in creating a distinct cultural community that supports its members’ abstinence (Wilcox 1998). [Question #4. Which contributes to a shared and necessary sense of belonging?] Emotional RestraintStarting in boyhood, many men learn that they should avoid stereotypical feminine characteristics or behaviors and strive to be tough.Some do this by attempting to suppress emotions, thoughts, and behaviors potentially associated with vulnerability. Because of the stigma attached to expressing his emotions, a man who experiences grief and sadness after the loss of a loved one, for example, might resort to substance use as a way of coping (Goodet al. 2000; Pollack 1998b). Men are more likely than women to respond to emotional stress by drinking (Geisner et al. 2004) and more likely to have a visceral response to alcohol-related cues when experiencing negative emotions (Nesic and Duka 2006). Even men classified as mild to moderate social drinkers report significantly more alcohol craving as the result of negative emotional states than women (Chaplin et al. 2008).
Many men have problems both identifying and expressing feelings, each of which has negative consequences. Difficulty identifying emotions can increase trait anxiety among men (Wong et al. 2006). Unlike women, men often do not develop an adequate vocabulary for expressing feelings; instead, they express them nonverbally (e.g., through violent actions or withdrawal) or suppress them (e.g., through substance use). Certain emotional states (e.g.,anger or sadness) may be predictive of violence toward partners, even after controlling for gender role stress ( Jakupcak 2003). These problems appear to be pronounced among men with substance use disorders, who often have difficulty recognizing and expressing certain feelings—such as hurt or vulnerability—that might be repressed and out of the individual’s awareness. Alexithymia (the inability to experience and/or communicate feelings) is not unusual in substance abuse treatment populations. In one sample of men entering treatment for alcohol dependency, 30 percent met criteria for this disorder (Evren et al. 2008). [Question #6. The inability to experience and communicate feelings?] Competition and SuccessCompetition can be a fun and important aspect of recreational activities and a positive attribute in various professional and business settings, but it is also a significant source of stress associated with increased substance use (Blazina and Watkins 1996). Only so many persons can be recognized as the best in any given domain. Boys and men who perceive themselves as falling short in an important area may attempt to suppress feelings of insecurity by using or abusing substances. Conversely, the effort and pressure often involved with being the best leads some men to unwindor celebrate their accomplishments with substance use. For example, higher success, power,and competition orientations are linked with increased alcohol problems among male college students (Magovcevic and Addis 2005),and male college athletes drink more than nonathletes (Martens et al. 2006). In this same vein, men are significantly more likely than women to respond to social stress by drinking(Lemke et al. 2008), and work-related stress is strongly associated with heavy drinking in men (Siegrist and Rodel 2006). The possible tension of living up to various concepts of masculinity likely contributes to, but does not solely cause, a man’s use or abuse of substances.
Aggressiveness, Fearlessness, and InvulnerabilityMen are often socialized to be aggressive and to appear fearless and invulnerable. To prove their masculinity, some men engage in reckless behaviors, including consuming large quantities of alcohol or drugs. The desire to take risks and the need to avoid showing weakness can affect men’s health-related beliefs and behaviors (Courtenay 2000, 2003; Lejuez et al.2004). Alcohol is also associated with increased aggression among men, and this effect may be stronger for men than for women. For example, Giancola (2002a) found that alcohol,when combined with higher levels of irritability, led to more aggressive behavior in men but not women. Illicit drug use may have a similar effect, given that some drugs (notably stimulants) are known to increase aggression and risk-taking behaviors.
[Question #7. Whose study showed that Alcohol, when combined with higher levels of irritability,leads to more aggressive behavior in men; but not in women?] As a group, men do not seek health care during illness or following injury nearly as often as women do (Addis and Mahalik 2003;Courtenay 2003; Sandman et al. 2000). Men are also more likely than women to engage in risky sexual behavior but less likely to take preventive measures (e.g., performing self-examinations for cancer, using sunscreen,wearing seat belts or helmets, not using addictive substances). These behaviors contribute to the higher death rate among men for all leading causes of death, as well as their shorter life spans compared with women (Case and Paxson 2005; Courtenay 1998; Eisler 1995;Waldron 2005). Additionally, some frameworks of masculinity can exacerbate medical conditions by increasing stress. This could partially explain why Hunt and colleagues (2007)found decreased death rates from coronary heart disease among men who scored higheron measures of feminine traits, despite there being no similar findings for women. Sexual AccomplishmentThe gender socialization process can cause men many problems related to sexuality. Many American men learn from an early age that identifying with girls, women, or anything feminine is not socially appropriate, and emotional intimacy may be characterized as feminine. At the same time, sexual conquest is often presented as an expression of real masculinity. Fear of femininity drives some men to become counterdependent and emotionally vulnerable to no one; in some cases, they emotionally disconnect from others and start to view sex as an achievement or a goal.
Men who hold this outlook on sexuality can have problems with what Good and Sherrod(1997) call “non relational sex,” or “the tendency to experience sex primarily as lust without any requirements for relational intimacy or emotional attachment” (p. 181). Having multiple partners with whom little communication is shared can result in unwanted pregnancies,higher risk of exposure to sexually transmitted diseases, and the spreading of diseases to multiple partners. Such behaviors add to growing public health problems. Men who engage in non relational sex can find intimacy difficult and relationship-building with members of either sex challenging. Men’s use of alcohol and drugs may be linked to their desire to fulfill male gender role expectations of power, dominance, and control over women. Research bears this out. Men who believe they have consumed alcohol are more likely to be aroused by violent sexual images or fantasies (Roehrich and Kinder 1991),and as they consume greater amounts of alcohol, their sexual fantasies are more likely toinvolve control over others (McClelland et al.1972). Greater alcohol consumption is also associated with a greater likelihood of sexual aggression among men (Peterson et al. 2009),as well as increased violence toward intimate partners (Foran and O’Leary 2008), both of which are discussed in detail in Chapter 4. A related aspect of this definition of masculinity is heterosexism —the assumption that heterosexual behavior is natural and therefore homosexual men are less masculine. Despite sexual orientation being a separate issue from gender identity, traditional concepts of masculinity equate the two. Heterosexual men may feel that their masculinity is threatened by homosexual behavior, resulting in homophobia(i.e., fear of homosexuality and homosexual persons)—which further contributes to prejudice against gay men and pressures them to at least appear to conform to heterosexual norms. Independence and Self-SufficiencyMen are expected to be independent and able to take care of themselves with little or no help from others. Help-seeking for many men implies dependence, vulnerability, or even submission to someone with more knowledge,such as a healthcare professional. The negative mental and physical health effects of internalizing this masculine role, which is perpetuated by cultural messages about masculinity and health, can be seen in men’s underutilization of healthcare resources—including behavioral health services (Add is and Mahalik 2003;Berger et al. 2005; Biddle et al. 2004). Men have significantly greater self-stigma related to help-seeking (i.e., believing that seeking help will decrease their self-confidence, cause them to doubt their abilities, and decrease their feelings of worth) than do women (Vogel et al.2006). In addition, conformity with male gender norms of self-reliance is associated with increased psychological distress and less willingness to seek help for psychological problems (Mahalik et al. 2003b).
These attitudes toward help-seeking also affect men’s interactions with primary care providers. Despite having a shorter life expectancy than women, men see their physicians less often (Cherry and Woodwell 2002) and ask fewer questions than female patients (Courtenay 2000). Compounding this problem, physicians make less effort to warn male patients about health risks (Foote et al. 1996). Men consume considerably more alcohol and drugs than women and are thus more likely to have substance use disorders (Grant et al.2005; SAMHSA 2009; von Sydow et al. 2001; von Sydow et al. 2002). However, men—particularly heterosexual men—are less likely than women to seek help for substance abuse (Addis and Mahalik 2003; Grella et al. 2009a). What might explain this discrepancy? Physical differences between the sexes could partially account for the variance in substance use and abuse, as could the socialization process for men and its resulting framework of masculinity. These may also contribute to differences in help-seeking behavior (Isenhart 2001; Williams and Ricciardelli 1999): men with substance use disorders are more likely than women to state that they can handle the problem on their own as a reason for not seeking treatment, whereas women’s reasons tend toward concerns about what others might think or lack of time (U.S. Department of Health and Human Services, SAMHSA, OAS 2009a). Acknowledging their illness (such as substance dependence) can cause men to feel helpless—a feeling that directly contradicts societal messages about masculinity (Good et al. 2000;Pollack 1995, 1998b). As Isenhart (2001) notes, “given this relationship between alcohol and masculinity, when a man is asked (or told)to give up alcohol, he may feel like he is giving up part of his masculine identity” (p. 250).Some men see health-sustaining practices (e.g.,having annual physicals, getting health screenings, performing health self-assessments) as unnecessary or humiliating. The Value of Gender RolesGender roles are neither all good nor all bad,and they vary according to social role (e.g., a man’s role as a father differs from his role as a son), age, and cultural background. Some components are useful, especially in specific situations. For example, men aligned with more traditional masculine roles may have strengths in such areas as logical thinking,problem-solving, risk-taking, anger expression,and assertive behavior. These traits can be particularly useful in times of crisis (Betcherand Pollack 1993; Levant 1995), enabling him to remain calm and problem-focused or to surrender his personal safety for the greater duty of protecting and providing for his family,community, or country (Good and Sherrod 2001). Conformity to male gender norms also fosters “acceptance from social groups, and[provides] social and financial rewards as a result” (Mahalik et al. 2005, p. 662). For men of color, adherence to gender roles can be a source of pride closely related to their cultural identity, helping protect them against racial and ethnic oppression and stigma (Levant etal. 1998; Ojeda et al. 2008; Saez et al. 2009).
[Question #8. Gender roles do not vary according to social role. True/False?] Gender Role Conflict and Masculine Role StressSeveral models attempt to explain how men become socialized. Among these are the theories of gender role conflict (O’Neil et al. 1995) and masculine role stress (Eisler and Skidmore 1987; Eisler et al. 1988), which focus on the negative consequences experienced by men who endorse particular beliefs regarding masculinity (Addis and Mahalik 2003; Good and Sherrod 2001; Pederson and Vogel 2007).
Gender role conflict occurs “when rigid, sexist,or restrictive gender roles result in personal restrictions, devaluation, or violation of others or self ” (O’Neil et al. 1995, pp. 166–167). This conflict can be experienced at a cognitive,emotional, or behavioral level, and may be conscious or unconscious.The Gender role Conflict Scale developed by O’Neil and colleagues (1986) gauges gender role conflict in four areas: success, power, and competition issues; restrictive emotionality; restrictive sexual and affectionate behavior between men; and conflict between work and family relations. As with gender role conflict, the theory of masculine role stress views the socialization of men from a cultural lens. Eisler (1995) notes that: Masculine gender role stress may arise from excessive commitment to and reliance on certain culturally approved masculine schema that limit the range of coping strategies employable in any particular situation…. Masculine gender role stress may also arise from the belief that one is not living up to culturally sanctioned gender role behavior. Men may experience stress if they feel that they have acted in an unmanly or feminine fashion. Many men are doubly stressed by experiencing fear or by feeling that they did not appear successful or tough enough in situations requiring masculine appearances of strength and invincibility (p. 213). Masculine role stress has been refined to include links to shame (discussed in Chapter 3),depression, and anxiety (Liu and Iwamoto 2006; Liu et al. 2005; Wong et al. 2006). [Question #9. “Rigid ,sexist, or restrictive gender roles result in personal restrictions, devaluation or violation of others or self”when:?] Men’s Substance AbuseRegardless of age or race, men use alcohol and drugs more frequently and in greater quantities than women. Similarly, young adults are more likely to use substances than are their older counterparts. The highest rate of illicit drug use is among young adult men, and the most common illicit drug used is marijuana. According to SAMHSA’s 2008 National Survey of Drug Use and Health (NSDUH),young adult men 18 to 25 years of age are also more likely to drink alcohol (64.3 percent)than their female counterparts (58.0 percent)(SAMHSA 2009). Binge drinking (a pattern of alcohol use that is more likely to result in alcohol-related problems) is likewise more prevalent among men. An earlier NSDUHstudy (SAMHSA 2005) indicated that eventhough 32.9 percent of men ages 21 and older reported prior-month binge alcohol use, only 14.7 percent of women in the same age group reported binge drinking in the prior month.People who binge drink have a higher incidence of alcohol-related problems (than those who do not binge drink), and men are more likely to binge drink than women, so counselors need to be aware, particularly when working with younger male clients, that binge drinking may be part of the individual’s drinking pattern.
[Question #10. The most common illicit drug used is :?] [Question #11. The substance used more frequently and in greater quantities is :] Perhaps reflecting these differences in use,American men are two to five times more likely to develop a substance use disorder than women (Brady and Randall 1999; Johnson and Glassman 1998; SAMHSA 2008;SAMHSA, OAS 2004a). In fact, in developed nations around the world, men experience greater mortality and morbidity from alcohol and tobacco use than women, due in part to greater rates of use (Lopez 2004). Worldwide,the health burden for substance use disorders is more than three times greater for men than women (World Health Organization 2004).The economic cost of men’s substance abuse is greater as well; men who abuse substances have more criminal justice system involvement than women who abuse substances, and because men are more likely to have jobs, they more often require disability payments (Harwood et al. 1998; Oggins et al. 2001; Timko etal. 2009). When men receive substance abuse treatment, taxpayers benefit: For every dollar spent on treatment, an estimated $9.00 is saved in criminal justice, healthcare, welfare,and disability costs (Harwood et al. 1998). Given the chance, men and women are equally as likely to use substances. However, men may be more likely than women to use and abuse them largely because they have more opportunities to do so (van Etten et al. 1999). This could, in part, account for higher rates of abuse and dependence among men. Men also generally begin using alcohol and drugs at an earlier age than women (SAMHSA 2005). Understanding how socially constructed gender role expectations affect some men’s choice of substances and attitudes toward treatment can help behavioral health service providers choose more effective strategies. Alcohol consumption, in particular, can be tied to ideas about masculinity and appropriately masculine activities. For young men, a first drink or first episode of drunkenness is often a rite of passage (Blazina and Watkins 1996; Hunt et al.2005), and drinking is commonly seen as a form of male bonding (West 2001). Such traditional ideas linking masculinity to drinking are prevalent across cultures (Heath 2000) and are associated with greater alcohol consumption among college men (Blazina and Watkins1996; West 2001) and military person-nel/veterans (Burda et al. 1992; West 2001). Men also respond differently than women to certain substances, and some substances have effects in men that they do not have in women(see Chapter 3). For example, when men and women think about cocaine cravings, their neural responses differ (Kilts et al. 2004); men who use cocaine are also more likely than women to state that cocaine increases their sex drive and that they have more sex when using cocaine (Washton 2009). Findings such as these suggest the possible usefulness of gender-specific treatment approaches for cocaine dependence and other substances of abuse. As with cocaine, there are differences between the sexes in both methamphetamine and opioid dependence. Men show greater loss of mental faculties relating to executive function and memory than women, and these effects persist even after abstinence (Ersche et al. 2006). Men may use or start to abuse substances for different reasons than women, and male institutions (e.g., fraternities, amateur sports teams) often encourage alcohol use (Brooks 2001). Men who cannot talk about their feelings or manage them constructively sometimes use substances to deal with difficult emotions. Shame, especially, can limit help-seeking behaviors for substance use and mental disorders (Brooks 2001; Pollack 1998b). 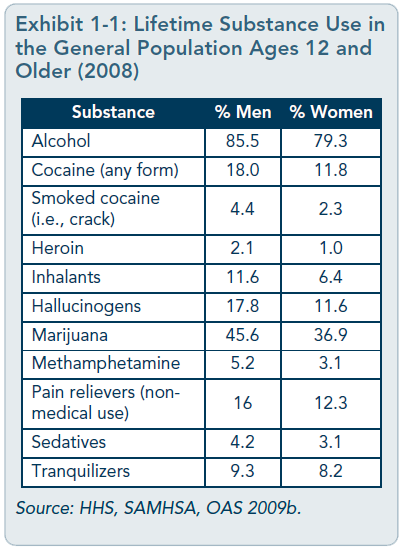 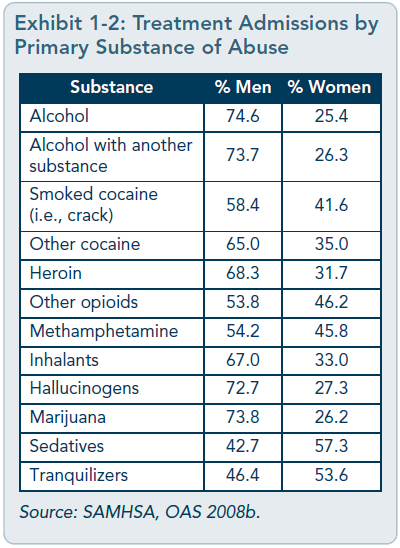 SAMHSA’s 2008 NSDUH established rates of lifetime use of substances for men and women (Exhibit 1-1); it found that 12 percent of menages 18 and older met criteria for a substance use disorder in the past year compared with 6.3 percent of women (SAMHSA 2009). SAMHSA’s 2006 Treatment Episode DataSet (SAMHSA, OAS 2008b) revealed differences in substance abuse patterns and preferred substances of abuse between men and women who entered substance abuse treatment programs funded through State agencies (Exhibit 1-2). For all drugs listed save sedatives and tranquilizers, most treatment-seekers were male. However, data reported in the exhibit are for the primary substance of abuse,which was not necessarily the only substance a person abused. State of the FieldSubstance abuse treatment was designed for a largely male client population, and greater numbers of men than women continue to be treated in a variety of behavioral health settings.Additionally, much of the research on substance abuse treatment has been conducted with male participants; nevertheless, it has not examined the specific, unique issues of men (e.g., their health, psychological, cultural, and social needs)as related to substance abuse and its treatment. There is a difference between designing a substance abuse treatment intervention for a population—the majority of whom are men—and designing one specifically to address factors that distinguish male from female clients.The study of men’s issues is a growing field, and as researchers focus on issues specific to men, our knowledge base—and thus our ability to design treatment interventions for men—will increase.
In 2006, 68.2 percent of admissions to substance abuse treatment programs receiving State agency funds were men (SAMHSA,OAS 2008b). However, data from 2005 show that only 25 percent of programs offered any type of specialized services for adult men (OAS2007a). These data exclude treatment programs for incarcerated clients, an even greater percentage of whom are male. In 2003, the Addiction Technology Transfer Centers (ATTCs) began offering two trainings related to men’s issues in treatment: “Men in Therapy” and “Anger Management”(http://www.attcnetwork.org/learn/education/dasp.asp). Trainings in substance abuse treatment specific to men are also available from other sources, such as the “Counseling Alcohol and Drug Dependent Men” training from the Distance Learning Center for Addiction Studies (http://www.dlcas.com). Men in general,regardless of age or cultural background, are less likely than women to seek treatment and more likely to leave treatment early, so motivational interviewing and treatment engagement skills should be a primary focus when training staff members who treat men. [Question #12.The trainings offered by Addiction Technology TransferCenters (ATTCs) related to men’s issues in treatment include:] Audience for This TIPBecause men who have substance abuse problems are a large and diverse group of people,this TIP will be useful to a broad audience of behavioral health service providers, including:
|
|
|
Addressing Behavioral Health Needs of Men: Substance Abuse > Chapter 1 - Introduction
Page Last Modified On: September 29, 2022, 02:48 PM
|
|